
Official websites use .gov
A
.gov
website belongs to an official government organization in the
United States.
Secure .gov websites use HTTPS
A
lock
(
) or
https://
means you’ve safely connected to the .gov website. Share sensitive
information only on official, secure websites.

Use of Certified Health IT and Methods to Enable Interoperability by U.S. Non-Federal Acute Care Hospitals, 2019
No. 54 | February 2021
Over the past decade, a number of federal health IT policies (1) have sought to advance the interoperable exchange of electronic health information (EHI) between health care providers. In response to these federal initiatives, health care organizations adopted a number of methods to exchange information and upgraded to 2015 Edition certified electronic health record (EHR) technology (2-3). The 21st Century Cures Act (Cures Act) (4) sought to improve the flow and exchange of EHI by defining “information blocking” and established penalties for those who engage in this practice. The Cures Act also sought to enhance the usability of health IT and the creation of a Trusted Exchange Framework and Common Agreement (TEFCA) to improve data sharing between health information networks (5). As the Office of the National Coordinator for Health IT (ONC) and the health IT industry begin to implement these policies, it will be important to track their impacts. This data brief uses nationally representative survey data from the 2019 American Hospital Association IT Supplement to describe the methods hospitals used to exchange or search for EHI. It also presents hospitals’ participation rates in health information exchanges (HIEs), variation in HIE participation by hospital type, and barriers to interoperability.
Highlights
- About 70 percent of hospitals reported integrating data into their EHR – a nearly 15 percent increase from 2018.
- A majority of hospitals used a mix of electronic and non-electronic methods to exchange summary of care records, however use of electronic third party methods Health Information Service Providers (HISPs), HIEs, and vendor networks increased in 2019.
- The proportion of hospitals that used a national network to find (or query) patient health information increased by nearly 40 percent between 2018 and 2019.
About 70 percent of hospitals reported integrating data into their EHR – a nearly 15 percent increase from 2018.
Figure 1: Percent of U.S. non-federal acute care hospitals that electronically find patient health information, and send, receive, and integrate patient summary of care records from sources outside their health system, 2014-2019.
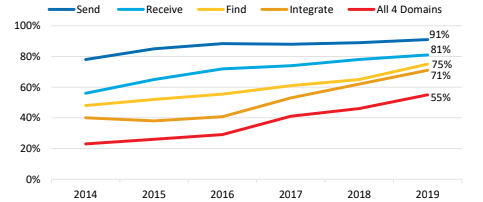
Note: See Appendix Table A2 for specific data points for all years.
- More than half of hospitals performed all four domains of interoperability (e.g., send, receive, find, integrate).
- Three-quarters of hospitals reported electronically finding (or querying) patient health information from sources outside their health system in 2019.
About nine in 10 hospitals nationwide had 2015 Edition Certified EHR Technology in 2019.
Figure 2: Percent of U.S. non-federal acute care hospitals that have a 2015 Edition Certified EHR by hospital size, 2017-2019.
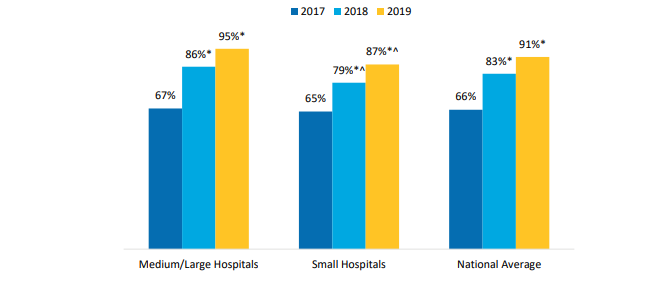
Note: *Significantly different from previous year (p<0.05). ^Statistically significant from medium/large hospitals (p<0.05). See Appendix Table A3 for breakdown by additional hospital characteristics.
- The proportion of small and medium/large hospitals that had a 2015 Edition Certified EHR increased between 2018 and 2019.
- Fewer independent, small, rural, and Critical Access Hospitals (CAHs) had a 2015 Edition Certified EHR compared to their counterparts in 2019 (see Appendix Table A3).
Health Information Service Providers (HISPs) were the most common electronic method used by hospitals for sending and receiving summary of care records in 2019.
Table 1: Percent of U.S. non-federal acute care hospitals that often or sometimes send or receive summary of care records with sources outside their hospital system by method, 2018-2019.
| Send | Receive | |||
|---|---|---|---|---|
| Methods | 2018 | 2019 | 2018 | 2019 |
| Non-Electronic Method | ||||
| Mail or fax | 71% | 68%* | 76% | 76% |
| eFax using EHR | 66% | 70%* | 52% | 56%* |
| Electronic Method Not Using Third-Party or Network | ||||
| Provider portal that enables viewing of another organizations’ EHR system | 49% | 55%* | 37% | 41%* |
| Interface connection between EHR systems (e.g. HL7 interface) | 42% | 45% | 30% | 31% |
| Access to other organizations’ EHR system using login credentials | 37% | 45%* | 26% | 26% |
| Electronic Method Using a Third-Party or Network | ||||
| HISPs that enables messaging via DIRECT protocol | 61% | 65%* | 49% | 55%* |
| State, regional, or local HIE | 59% | 62%* | 46% | 51%* |
| EHR vendor-based network that enables exchange between users of a single EHR vendor | 43% | 47%* | 41% | 47%* |
| National networks that enables exchange across different EHR vendors (e.g. CommonWell, Carequality) | 35% | 41%* | 32% | 40%* |
Note: *Significantly different from previous year (p<0.05).
- The proportion of hospitals using third parties and networks to exchange summary of care records increased between 2018 and 2019.
- Mail or fax continues to be the most common method for exchanging summary of care records – about seven in 10 hospitals used mail or fax to send and receive health information in 2019.
- The proportion of hospitals using provider portals to send and receive summary of care records increased between 2018 and 2019.
A majority of hospitals reported using a mix of electronic and non-electronic methods for exchanging summary of care records in 2019.
Figure 3: Percent of U.S. non-federal acute care hospitals that often or sometimes receive/send summary of care records by method type, 2017- 2019
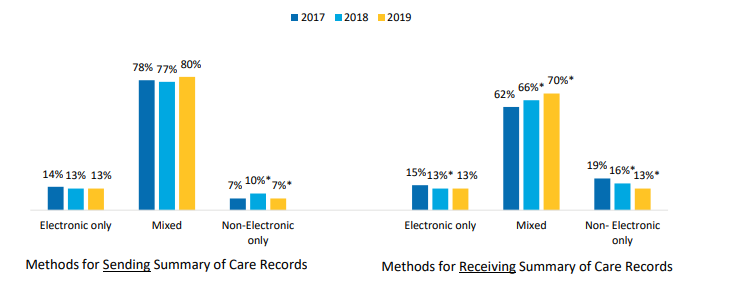
Notes: *Significantly different from a corresponding category in previous year (p<0.05).
- In 2019, 80 percent of hospitals used a combination of electronic and non-electronic methods to send summary of care records and 70 percent used a combination of methods to receive summary of care records.
- About one in 10 hospitals used only electronic methods for sending and receiving summary of care records.
- The proportion of hospitals that used only non-electronic methods to send and receive summary of care records decreased between 2018 and 2019.
The proportion of hospitals that used a national network to find (or query) patient health information increased by nearly 40 percent in 2019.
Figure 4: Methods used to electronically find (or query) for patients’ health information, 2018-2019.
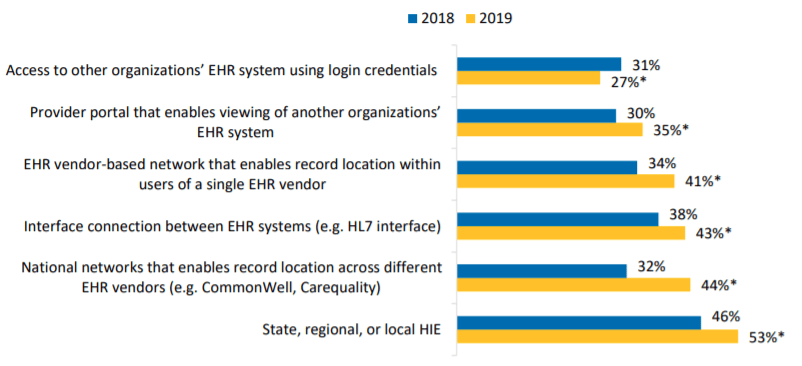
Notes: *Significantly different from a corresponding category in previous year (p<0.05).
- State, regional, or local HIEs were the most common method used to electronically find (or query) patient health information from outside sources.
- More than half of hospitals used state, regional or local HIEs to electronically find (or query) patient health information from outside sources – a statistically significant increase from 2018
- About four in 10 hospitals used provider portals, interface connections between EHR systems, and national networks to electronically find (or query) patients’ health information in 2019.
- The proportion of hospitals that accessed another organization’s EHRs using login credentials to find (or query) patient health information decreased in 2019.
The average number of electronic methods hospitals use to send, receive, and find (or query) health information increased between 2018 and 2019.
Figure 5: Average number of electronic methods hospitals use to send, receive, and find (or query) health information, 2018-201
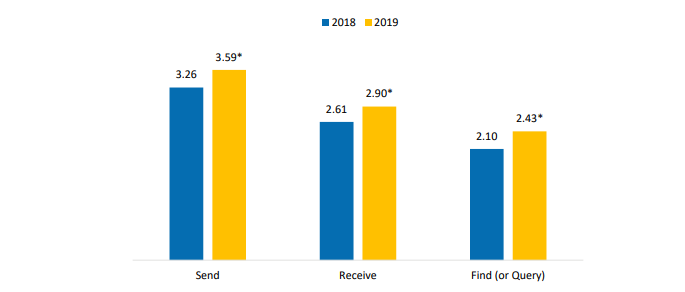
Notes: *Significantly different from a corresponding category in previous year (p<0.05).
- On average, hospitals used about three different electronic methods for sending (3.59) and receiving (2.90) summary of care records in 2019.
- On average, hospitals used about two different electronic methods to find (or query) (2.43) patient health information in 2019.
Nearly half of hospitals participated in more than one national network in 2019.
Table 2: Hospitals’ participation in national networks, 2018-2019.
| Overall National Network Participation | 2018 | 2019 |
|---|---|---|
| Percent of Hospitals that Participate in Any Network | 57% | 69%* |
| Percent of Hospitals that Participate in More than One Network | 33% | 48%* |
| Average Number of Networks | 1.21 | 1.67* |
| National Network | Percent | |
| Single-EHR vendor network | 32% | 41%* |
| e-Health Exchange | 25% | 27%* |
| DirectTrust | 21% | 38%* |
| Carequality | 20% | 31%* |
| CommonWell Health Alliance | 19% | 26%* |
Notes: *Significantly different from previous year (p<0.05). This table presents the top 5 national networks that hospitals reported participating in most frequently, additional networks were included in the calculation of the overall participation metrics. Please note, in 2018 and 2019, the survey described e-Health Exchange and Carequality as being operated by The Sequoia Project, however, these organizations split into separate entities in 2018.
- The average number of national networks hospitals participated in increased between 2018 and 2019.
- Single-EHR vendor networks were the most commonly participated network among hospitals.
- About one in three hospitals participated in CommonWell Health Alliance, Carequality, and e-Health Exchange, respectively.
More than half of hospitals participated in both a national network and a state, regional, or local HIE – a statistically significant increase from 2018.
Figure 6: Percent of U.S. non-federal acute care hospitals that participate in national and state, regional, or local health information networks, 2018- 2019
Notes: *Significantly different from previous year (p<0.05)
- About seven in 10 hospitals reported participating in national network – a 21 percent increase in 2019.
- One in 10 hospitals did not participate in a national network or a state, regional, or local HIE – a statistically significant decrease from 2018.
- About three-quarters of hospitals connected to a state, regional, or local HIE in 2019.
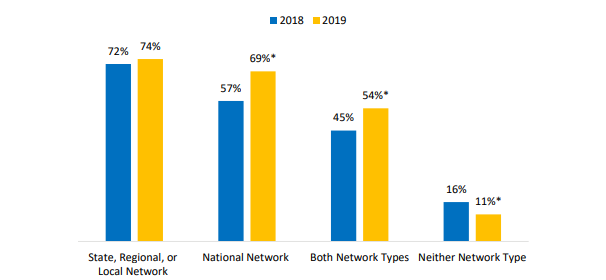
The proportion of small, rural, and CAHs that participated in both national and state, regional or local health information networks was lower compared to their counterparts.
Table 3: Percent of U.S. non-federal acute care hospitals that participate in national and state, regional, or local health information networks by hospital type, 2019.
| Type of Network | Medium-Large | Small | Suburban-Urban | Rural | Non-CAH | CAH |
|---|---|---|---|---|---|---|
| State, Regional, or Local Network | 80% | 68%* | 78% | 68%* | 76% | 68%* |
| National Network | 75% | 63%* | 74% | 62%* | 73% | 59%* |
| Both Network Types | 61% | 47%* | 59% | 46%* | 57% | 46%* |
| Neither Network Type | 5% | 17%* | 7% | 17%* | 8% | 19%* |
Notes: *Significantly different from a corresponding category presented in the column to the left (p<0.05).)
- Less than half of small, rural, and CAHs participated in both national and state, regional, or local health information networks.
- Small, rural, and CAHs were more likely to report participating in neither a national network nor a state, regional, or local HIE compared to their counterparts.
More than 70 percent of hospitals reported challenges exchanging data across different vendor platforms.
Table 4: Percent of U.S. non-federal acute care hospitals that experienced barriers when trying to electronically send, receive, or find health information to/from other care settings or organizations, 2019.
| Percent | |
|---|---|
| Barriers related to electronically sending patient health information | |
| Difficult to find providers’ Direct address | 58% |
| Exchange partners’ EHR system lacks capability to receive data | 59% |
| Exchange partners’ we would like to send data to do not have an EHR or other electronic system to receive data | 48% |
| Many recipients of care summaries report that the information is not useful | 40% |
| Cumbersome workflow to send the information from our EHR system | 24% |
| The complexity of state and federal privacy and security regulations makes it difficult for us to determine whether it is permissible to electronically exchange patient health information | 12% |
| Lacking the technical capability to electronically send patient health information to outside providers or other sources | 8% |
| Barriers related to electronically receiving patient health information | |
| There are providers whom we share patients with that don’t typically exchange patient data with us | 66% |
| Difficult to match or identify the correct patient between systems | 46% |
| We lack the technical capability to electronically receive patient health information from outside providers or other sources | 17% |
| Other barriers related to exchanging patient health information | |
| Greater challenges exchanging data across different vendor platforms | 73% |
| Paying additional costs to exchange with organizations outside our system | 42% |
| Develop customized interfaces in order to electronically exchange health information | 48% |
- Nearly 60 percent of hospitals reported having difficulty finding provider’s address and their exchange partner’s EHR lacking capability to receive data.
- Less than one in 10 hospitals reported lacking the capability to electronically send patient health information.
- More than 65 percent of hospitals reported there are providers who they share patients with that do not typically exchange data.
- Nearly half of hospitals (46 percent) had difficulty identifying or matching patients between systems.
The most common change hospitals plan to make to their EHR in the next 18 months is to optimize functionalities of new releases.
Figure 7: Percent of U.S. non-federal acute care hospitals that plan to make changes to their EHR system in the next 18 months, 2017-2019.
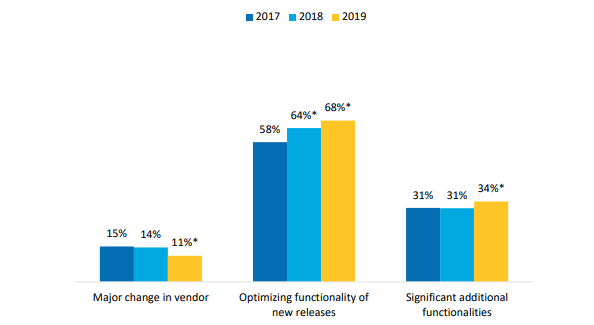
Note: *Significantly different from previous year (p<0.05).
- About a third of hospitals reported plans to add functionalities to their EHR in the next 18 months.
- One in 10 hospitals reported plans to change their EHR vendor in the next 18 months.
- The percent of hospitals planning to optimize functionalities of their EHR has increased each year since 2017.
Summary
This data brief highlights hospitals’ progress in performing the four domains of interoperability. These domains demonstrate whether hospitals routinely find, send, receive, and integrate EHI with sources outside their health system. Since 2014, hospitals’ rates of performing these activities has steadily increased. In 2019, most hospitals were able to send (91%) and receive (81%) summary of care records with sources outside their health system. More hospitals also reported that they routinely find (or query) and integrate patient health information from outside sources. About seven in ten hospitals reported being able to perform these domains in 2019 – a nearly 15 percent increase from 2018.
Increased rates of interoperability coincided with increases in hospitals’ adoption of EHRs certified to the 2015 Edition. The 2015 Edition contained enhanced certification criteria, standards, and implementation specifications to facilitate greater interoperability among health care providers. In 2019, about nine in 10 hospitals reported having 2015 Edition Certified EHR Technology.
Despite improvements in interoperability, few hospitals relied solely on electronic methods to exchange patient health information. Most hospitals still use a combination of electronic and non-electronic methods to send (80%) and receive (70%) summary of care records. A majority of hospitals used multiple methods to exchange health information. For example, hospitals on average reported using three different methods to send and receive summary of care records. The most frequently used electronic methods to exchange data involved third parties, such as HISPs and national and regional health information networks.
Additionally, hospitals reported using multiple methods to electronically find (or query) patient health information. State, regional or local HIEs were the most commonly used method for finding health information (53%), followed by EHR connectionsto national networks (44%), and interface connections between EHR systems (43%). However, fewer hospitals accessed other organization’s EHR using login credentials in 2019. Hospitals’ participation in national networks increased. Nearly 70 percent of hospitals reported participating in a national network in 2019. Almost half of hospitals participated in more than one network. Hospitals’ participation in five of the six networks reviewed increased between 2018 and 2019. Notably, however, there were significant differences in participation rates by hospital characteristics. Small, rural, and CAHs significantly lagged behind their counterparts in participation with national networks and state, regional, or local HIEs.
Hospitals reported barriers to exchange in 2019. About seven in 10 hospitals reported barriers related to information blocking, such as difficulty exchanging data across different vendor platforms and hospitals having providers whom they share patients with that do not typically exchange patient data. Moreover, over half of hospitals reported difficulty finding a provider’s Direct address and that their exchange partners’ EHR lacked the capability to electronically receive data.
ONC is working to improve the flow of EHI between patients, health care providers, and health information networks. In May 2020, ONC released its Cures Act Final Rule which adopted a set of certification requirements that focus on standardized, transparent, and pro-competitive practices to support the access, exchange, and use of EHI (6). The rule defined information blocking as well as eight exceptions that are considered reasonable and necessary activities that do not constitute information blocking (7). The final rule also requires health IT to provide a standardized set of health data elements (e.g. patient demographics, clinical notes, allergies, and medications) that are essential for exchange. These data elements are outlined in the United States Core Data for Interoperability (USCDI) and can help with patient matching between systems and ensure that data in summary of care documents can be effectively understood when it is received (8). ONC has also begun Year 2 of its cooperative agreement with the Sequoia Project to serve as the Recognized Coordinating Entity to support implementation of TEFCA, which will enable exchange of clinical data across qualified health information networks (QHINS) (9). Together, these efforts have the potential to improve access and exchange of EHI.
Definitions
Non-federal acute care hospital: Hospitals that meet the following criteria: acute care general medical and surgical, children’s general, and cancer hospitals owned by private/not-for-profit, investor-owned/for-profit, or state/local government and located within the 50 states and District of Columbia.
Interoperability: The ability of a system to exchange electronic health information with and use electronic health information from other systems without special effort on the part of the user (3). This brief further specifies interoperability as the ability for health systems to electronically send, receive, find, and use health information with other electronic systems outside their organization.
Integrate: Whether the EHR integrates summary of care record received electronically (not eFax) from providers or sources outside your hospital system/organization without the need for manual entry.
Find: Whether providers at your hospital query electronically for patients’ health information (e.g., medications, outside encounters) from sources outside of your organization or hospital system.
Small hospital: Non-federal acute care hospitals of bed sizes of 100 or less.
Rural hospital: Hospitals located in a non-metropolitan statistical area.
Critical Access Hospital: Hospitals with less than 25 beds and at least 35 miles away from another general or critical access hospital. Health information exchange (HIE): State, regional, or local health information network. This does not include local proprietary or enterprise networks.
Health information service provider (HISP): HISPs are network service operators that enable nationwide clinical data exchange using Direct Secure Messaging.
National network: Health information networks that are nationwide in scope. This includes multi-EHR vendor networks (e.g. Commonwell or e-Health Exchange) which can be used to exchange health information either directly through an EHR or health information exchange (HIE) vendor.
2015 Edition Certified Electronic Health Record (EHR) Technology: An EHR system that meets certification criteria requirements established by the U.S. Department of Health and Human Services. These criteria establish the required capabilities, standards, and implementation specifications that health information technology needs to meet in order to become certified under the ONC Health IT Certification Program. Certified health IT products can be used for participation in CMS quality reporting programs and State Promoting Interoperability Programs.
Data Source and Methods
Data are from the American Hospital Association (AHA) Information Technology (IT) Supplement to the AHA Annual Survey. Since 2008, ONC has partnered with the AHA to measure the adoption and use of health IT in U.S. hospitals. ONC funded the 2018 AHA IT Supplement to track hospital adoption and use of EHRs and the exchange of clinical data.
The chief executive officer of each U.S. hospital was invited to participate in the survey regardless of AHA membership status. The person most knowledgeable about the hospital’s health IT (typically the chief information officer) was requested to provide the information via a mail survey or secure online site. Non-respondents received follow-up mailings and phone calls to encourage response.
The survey was fielded from the beginning of January 2020 to the end of June 2020. The response rate for non-federal acute care hospitals was 59 percent. A logistic regression model was used to predict the propensity of survey response as a function of hospital characteristics, including size, ownership, teaching status, system membership, and availability of a cardiac intensive care unit, urban status, and region. Hospital-level weights were derived by the inverse of the predicted propensity.
References
1. The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA), (Pub. L. No. 114 – 10, enacted April 16, 2015), Section 106(b)(1). https://www.congress.gov/114/statute/STATUTE-129/STATUTE-129-Pg87.pdf.
2. Pylypchuk Y., Johnson C., Patel V. (March 2020). State of Interoperability and Methods Used for Interoperable Exchange among U.S. Non-federal Acute Care Hospitals in 2018. ONC Data Brief, no.51. Office of the National Coordinator for Health Information Technology: Washington DC.
3. Office of the National Coordinator for Health IT. 2015 Edition Certified Health IT. https://healthit.gov/certification-health-it/
4. 21st Century Cures Act, section 4006. https://www.congress.gov/114/statute/STATUTE-130/STATUTE-130-Pg1033.pdf.
5. Office of the National Coordinator for Health IT. Trusted Exchange Framework and Common Agreement (TEFCA). https://healthit.gov/policy/tefca/
6. Office of the National Coordinator for Health IT. ONC Cures Act Final Rule. https://healthit.gov/wp-content/uploads/2025/07/ONCCuresActNPRM.pdf
7. Office of the National Coordinator for Health IT. Information Blocking. https://healthit.gov/information-blocking/
8. Office of the National Coordinator for Health IT. United States Core Data for Interoperability (USCDI). https://www.healthit.gov/isa/united-states-core-data-interoperability-uscdi
9. Berry, M. (May 26, 2020). A Look Ahead: Year Two for ONC and the Recognized Coordinating Entity for TEFCA. Health IT Buzz Blog. Available here: https://healthit.gov/blog/health-it/a-look-ahead-year-two-for-onc-and-the-recognized-coordinating-entity-for-tefca/
Acknowledgements
The authors are with the Office of Technology, within the Office of the National Coordinator for Health Information Technology. The data brief was drafted under the direction of Mera Choi, Director of the Technical Strategy and Analysis Division, and Talisha Searcy, Deputy Director of the Technical Strategy and Analysis Division.
Suggested Citation
Johnson C. & Pylypchuk Y. (February 2021). Use of Certified Health IT and Methods to Enable Interoperability by U.S. Non Federal Acute Care Hospitals, 2019. ONC Data Brief, no.54. Office of the National Coordinator for Health Information Technology: Washington DC.
Appendix Table A1: Survey questions assessing variation in interoperability among hospitals
| Question Text | Response Options |
|---|---|
| When a patient transitions to another care setting outside your organization or hospital system, how often are the following methods used to send a summary of care record? Please indicate how often each method is used across each row below. |
Often | Sometimes| Rarely | Never | Do not Know/NA Methods without intermediaries:
|
| When a patient transitions from another care setting outside your organization or hospital system, how often are the following methods used to receive a summary of care record? Please indicate how often each method is used across each row below. |
Often | Sometimes| Rarely | Never | Do not Know/NA Methods without intermediaries:
|
| Does your hospital query electronically for patients’ health information (e.g. medications, outside encounters) from sources outside of your organization or hospital system? Note: Hospitals that autoquery should respond “Yes. |
|
| How often are the following electronic methods used to search for (e.g., query or auto-query) and view patient health information from sources outside your organization or hospital system? Please indicate how often each method is used across each row below. |
Often | Sometimes | Rarely | Never | Don’t Know/NA
|
| Does your EHR integrate the information contained in summary of care records received electronically (not eFax) without the need for manual entry? Note: This refers to the ability to add or incorporate the information to the EHR without special effort (this does NOT refer to automatically adding data without provider review). This could be done using software to convert scanned documents into indexed, discrete data that can be integrated into EHR. |
|
| When does your hospital expect to switch to a 2015 certified EHR system? This refers to fully implementing the 2015 certified EHR system. |
|
| Please indicate your level of participation in a state, regional, and/or local health information exchange (HIE) or health information organization (HIO). Note: this does not refer to a private, enterprise network. |
|
| Which of the following national health information exchange networks does your hospital participate in? Check all that apply. |
National networks that enable record location and exchange across users of different EHRs
|
| Which of the following issues has your hospital experienced when trying to electronically (not eFax) send, receive or find (query) patient information to/from other care settings or organizations? Check all that apply. |
Barriers related to electronically sending patient health information
|
| What changes, if any, are you planning for your primary inpatient EMR/EHR system within the next 18 months? Please check all that apply. |
|
Appendix Table A2: Percent of U.S. non-federal acute care hospitals that electronically find patient health information, and send, receive, and integrate patient summary of care records from sources outside their health system, 2014-2019.
| Domains | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 |
|---|---|---|---|---|---|---|
| Send | 78% | 85%* | 88%* | 88% | 89% | 91% |
| Receive | 56% | 65%* | 72%* | 74% | 78%* | 81%* |
| Find | 48% | 52%* | 55%* | 61%* | 65%* | 75%* |
| Integrate | 40% | 38% | 41% | 53%* | 62%* | 71%* |
| All 4 Domains | 23% | 26%* | 29%* | 41%* | 46%* | 55%* |
Appendix Table A3: Percent of U.S. non-federal acute care hospitals that have a 2015 Edition Certified EHR by hospital size, 2017-2019.
| Hospital Characteristics | 2017 | 2018 | 2019 |
|---|---|---|---|
| Rural | 63%^ | 78%*^ | 88%*^ |
| Suburban/Urban | 68% | 86%* | 93%* |
| CAH | 66% | 78%*^ | 87%*^ |
| Non-CAH | 66% | 84%* | 93%* |
| System-Affiliated | 67%^ | 87%*^ | 94%*^ |
| Independent | 63% | 75%* | 85%* |