
“You Never Want to Go Back”: The Promise of Health IT
Dr. Vindell Washington | October 17, 2016

On Friday, October 14, 2016, Dr. Vindell Washington delivered a keynote address at the Association of Health Care Journalists’ (AHCJ) Journalism Workshop on Health Information Technology. The following are Dr. Washington’s remarks as prepared.
View Dr. Washington’s PowerPoint presentation here.
Good afternoon, journalists! Thank you, Julie, for that kind introduction. I would also like to thank Len and the Center for Excellence in Health Care Journalism for inviting me here to speak with you all today. You all have put together a terrific program and I am honored to be a part this workshop on health IT.
As you could see from our new video, we have been hard at work at the Office of the National Coordinator for Health IT — or ONC. Which is why I am so excited to be here with you this afternoon. Along those lines, I’d like to talk about 3 things today: First, I’d like to give you a bit of background on the work we do at ONC, second, I want to dive into how we are working today to unlock health data to build the foundation for a wide variety of health innovations, and finally third, I’ll close with a reflection on the promise of health IT.
Before we delve into those topics, I’m going to take you back a few decades— a time when I found my passion for health IT in an unlikely place. During my time as a Captain in the U.S. Army, I was assigned to support the 18th Airborne Corps. While deployed in Port-au-Prince, Haiti a superbly fit, 20-something fellow soldier, arrived at our doorstep an unusual symptom complex that we just didn’t recognize.
He came to our field hospital emergency department appearing generally ill with a rash and mild fever and he was clearly too sick to serve in theatre. We couldn’t figure out a diagnosis or appropriate treatment—or even how serious the situation might be.
After considering our options, we remembered our hospital commander had talked about a new gizmo that he had for this deployment. So, we set up a telecommunications kit on the roof of a Humvee and linked with our support unit, the Walter Reed National Military Medical Center in Washington, D.C. Infectious Disease and dermatology specialists there helped us to diagnosis the first case of porphyria of my career – a relatively rare, often genetic skin or nervous system disorder.
This connection with a premier institution 1400 miles away was invaluable and allowed us to properly diagnose and treat our patient. I remember, thinking at that time, “the way we think about practicing medicine will never be the same again. Once you have access to any technology that allows you to significantly improve patient outcomes, you never want to go back. Nor should you.
Fast forward a couple of decades and we’ve seen how true that is.
Our nation has made rapid, historic gains when it comes to the adoption and use of electronic health records just as you saw in our video. In 2009, most hospitals, doctors’ offices, and other health facilities captured patient care information on paper and shared this information primarily using fax machines. The tech revolution was well on its way in 2009 with a new and improved iPhone, Twitter moving into mainstream, streaming music, and Google’s Android all picking up steam.
The fact that healthcare was still a paper world eight years ago, is just incredible. And, as in so many other areas, going digital has a real impact. You’ll remember that there was a time when everyone had scores of doctor’s handwriting jokes. All the while many of us in healthcare knew even then that the errors in medicine due to illegible handwriting were more like horror stories. Many tragic errors were the result.
You’ll also remember a time when drug- allergy or basic drug-drug interactions being missed when there wasn’t an automated system as a backstop. Or when the physician’s ability that we sometimes now take for granted, to check an electronic record from home, or send it to a colleague in seconds—was just a dream.
In fact, there was a recent American Academy of Family Physicians website article where a Dr. Carl R. Olden, a family physician in Yakima, Washington, and a member of their board of directors, talked about the values of completing rounds remotely, reading x-rays remotely and managing a telemedicine visit with a child — in his digital practice and he spoke of what the changes meant for him.
These advances have real benefits for real patients. I saw it often while practicing emergency medicine in Baton Rouge as recently as this past January coordinating complex care across care sites with specialists in ways that were not possible in the past. So I can’t underscore just how important it is that nearly all hospitals and three quarters of physicians are now using certified electronic health records. And I want to emphasize that this progress did not just happen on its own. We have been able to make these incredible advances as a result of a deliberate choice – by the government and the private sector, to digitize healthcare in this country.
It started when ONC was established by Executive Order in 2004. In 2009, ONC was codified in the Health Information Technology for Economic and Clinical Health, or HITECH Act, which was part of the Recovery Act. HITECH charged ONC with coordinating nationwide efforts to adopt and use electronic health records, or EHRs, to facilitate the secure flow of electronic health information, and in order to promote the delivery of safer, more efficient, and higher quality care.
Now, it’s great that EHRs are part of the normal course of business for doctors and hospitals. But, today, I want to take you beyond the normal course of business. I want to talk about why this digital health foundation underpins virtually all the innovative health initiatives you are hearing about.
And if there is one thing about ONC that I want you all to remember as you walk away from here today, it is that ONC’s mission is to help unlock health data and put it to work on these initiatives.
Let’s start with delivery system reform. As many of you know HHS is working to move the focus from quantity to quality of care or from volume of treatments and procedures to the value of care delivered across the nation in three ways. First, we are changing how we pay doctors, so they can focus on the quality of care they provide, not the quantity of services they order. Second, we are making changes to help improve care, by encouraging better coordination and prioritizing wellness and prevention. Third, we are helping to unlock health care data to empower patients and to give doctors the data they need to provide the best possible care.
I’m sure for some of you writing about the general principles behind delivery system reform, the idea of value over volume or quality over quantity, is probably old hat at this point. But I have to say, the third leg of delivery system reform, the health IT leg, often times gets glazed over. When in reality, health IT is essential infrastructure that allows for this effort to be successful.
That’s why I’m so excited to talk with you about the final Quality Payment Program rule that we announced just this morning. This rule implements the “doc fix,” more formally known as the Medicare Access and CHIP Reauthorization Act, or MACRA. As many of you already know, this is a major step in transitioning how we pay for care in this country to reward quality. Just as a refresher, MACRA was supported by an overwhelmingly bipartisan majority in Congress, as well as patient groups and medical associations. It ended the Sustainable Growth Rate formula and, with it, 13 years of potential payment cliffs for Medicare doctors and clinicians.
When I was President of our private practice group in North Carolina, every year we ran scenarios of how we would survive with a 20% Medicare cut, while we simultaneously tried to figure whom we should plead our case. It was simply exasperating.
Our new program will reform Medicare payments for over 600,000 clinicians across the country and remove the awful uncertainty and I want to emphasize how much the Program relies on the seamless and secure flow of health data. Our collective goal throughout the QPP is to support the vision of a simpler approach to technology for providers; focused on advancing information sharing and better outcomes for patients.
Now, how are we doing that in this program?
Let me list a few key things where the new approach is different from the status quo. We are allowing doctors to select the measures that reflect how technology best suits their day-to-day practice. We are no longer requiring all-or-nothing EHR measurement for quality reporting. We are dramatically reducing the number of required metrics to report on the use of health IT, and focusing those that remain on improving the flow of health data, in areas like patient access to data—and providers ability to send and receive electronic information. We provide “bonus points” for doctors and practices that use certified health IT to perform practice improvement activities like population management or care coordination – because improving the coordination of care between teams of doctors, or monitoring the health of a whole panel of patients—or a whole community—or identifying those who need the most attention, before they show up in the emergency department—depends on health IT. Finally, we make clear that succeeding in Alternative Payment Models requires the effective use of technology. In short, the Quality Payment Program recognizes and rewards the fact that health IT is foundational to providing quality care.
But unlocking health data goes well beyond delivery system reform or the Quality Payment Program. From where I sit, I can’t tell you how often this work on the flow of electronic health information comes up across a wide range of the Administration’s top priorities. For example, the President’s Precision Medicine Initiative depends on making usable electronic health data readily available and easily transferable for patients, providers, and researchers. Or take the Cancer Moonshot. As Vice President Biden recently said, the flow of electronic health data is critical to accelerating efforts to cure cancer.
And finally, all of us in the Federal Government are doing what we can to combat the opioid crisis. One important, concrete step is sharing information from state prescription drug monitoring programs seamlessly with providers and at ONC, we are working with our partners to make these state and regional databases interoperable with the electronic health records that clinicians use in routine care. I can tell you from my personal experience as an emergency medicine doctor that is a critical step to their success.
This list goes on, but I think I’ve made my point—our work to unlock health data and put it to use is foundational to each and every one of these initiatives.
Now, some of you might be thinking, “that sounds great, but if this is so foundational, why haven’t I heard about it happening all the time in every care setting, on every smart phone, and on every home computer? We’ve spent a lot of time thinking about that question at ONC, to turn the vision into the on the ground reality.
We’ve landed on three key drivers of success. Number one – we need to ensure that unlocking the data is building the business case for information sharing. In other words, we need to use Medicare and other payment programs to reward the flow of information to improve care. Number two – we need to promote the use of common, federally recognized, national data standards. Ultimately, health technologies need to be able to speak the same language, or at least have reliable interpreters in the form of interfaces, to truly unleash the potential of all the electronic health care data that now exists in the ecosystem. And finally, and in my opinion most importantly, number three – we need to change the culture around access to information. This includes things like combating data blocking. Too often we are seeing health systems and vendors focusing competing on having access to data not delivering better care or applications, and it is holding back progress.
I’d like to focus on changing the culture around access to information for a minute. I hear confusion about HIPAA almost everywhere I go in this job. People insist that HIPAA makes it difficult, if not impossible, to move electronic health data when and where it is needed for patient care and health. I wish I could talk to every doc and patient in the country to tell them, “This just isn’t true.” But unfortunately, this misconception is widespread.
In reality, HIPAA not only protects personal health information from misuse, it also enables the access, use, and sharing of protected health information among and between providers and their health IT systems when and where it is needed for patient care. Interestingly, survey data tells us that consumers already believe this type of information exchange happens as a matter of course. Sadly, it doesn’t.
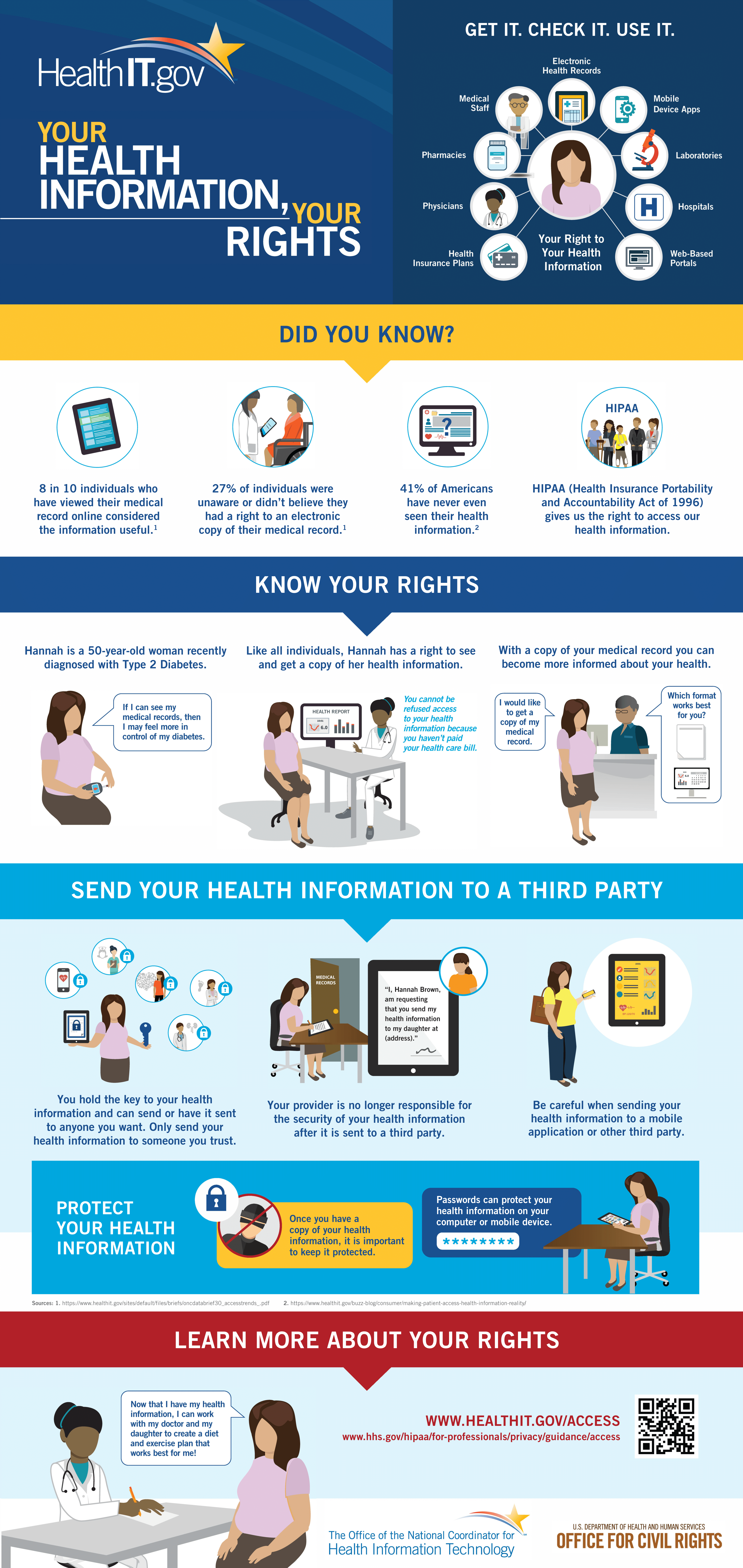
These misunderstandings of HIPAA and other business practices are inhibiting us from realizing the true potential for technology in supporting patients and clinicians. Providing an individual with easy access to their health information empowers them, it helps put them in control of decisions regarding their health and well-being, and it helps them actively partner with their care teams as well.
Individuals with access to their health information are better able to monitor chronic conditions, adhere to treatment plans, find and fix errors, and directly contribute their information to research. In fact, research has found that when individuals have access to, and use, their health information electronically, they feel a greater sense of trust in how their health information is being managed and in how providers are protecting their patient rights. And a recent ONC consumer survey found that over 8 in 10 individuals who had accessed their records online aid the information was useful.
So what are we doing to address this problem?
At ONC, we have worked with the HHS Office for Civil Rights, or OCR, to clarify individuals’ legal rights to access their data and transmit it to where they want. We recently adapted this guidance and developed a set of easy-to-understand educational tools in English and Spanish for consumers to understand these important rights, and exercise them. In addition to an easy-to-understand and easy-to-share infographic, we boiled down the legalese into plain language videos—highlighting important components of a patient’s legal right to access their health information.
{kind=link}
These videos can serve an important role in educating not only patients, but also the entire health system, about the facts when it comes to HIPAA. These videos are available at HealthIT.gov/Access and are being disseminated to health care providers and stakeholder organizations across the country.
When I found out I’d be speaking with you all today – I knew that I could not pass up on the opportunity to share these resources with you. You all play such a critical role in informing the public on a wide range of issues. I encourage you to visit HealthIT.gov/Access to learn more about your readers’ right to their health data and help us dispel with the myth that Americans do not have the right to access to their health information and to send it where they wish—from a family member to an app.
Now it is one thing to empower and encourage patients to retrieve and share their health data, but it is another challenge to ensure their doctors and hospitals are willing and able to share it with them. Thankfully, we have also seen tremendous progress on this front.
In fact we recently released data showing more hospitals than ever make information available electronically to patients. Specifically, the data show that nearly all of the nation’s hospitals provide patients with the ability to view their health information electronically. Close to 90% provide individuals the ability to download their health information. And almost 70% provide patients with the ability to view, download, and transmit their health information.
These are dramatic increases in a very short period of time. Both view and download availability have increased 70% compared to 2012 and the proportion of hospitals that provide all 3 capabilities increased 7-fold from 2013 estimates, where only 10% of the hospitals provided the same access.
Another statistic I like to highlight is that, now, all states have at least 40% of their hospitals providing patients with all three capabilities. By contrast, in 2013, no states had 40% or more of their hospitals with all 3 capabilities. I like to highlight that because it shows that we’re making great progress for patients throughout the country.
In addition to this exciting new data, I wanted to be sure to highlight a resource at ONC that I believe will be of particular interest in your reporting. And that is our handy web app which visualizes your state’s data statistics on a range of health IT topics including: EHR adoption, Health Information Exchange, health IT vendor market share, and programs funded by the HITECH Act. When visiting this site, you will be able to generate a custom report of the available state and national health IT estimates. So visit the site and explore some of the many other tools and open data resources we have to help localize this issue for your readers and, highlight some of the great progress that’s being made in your communities.
In closing, I wanted to share one more personal anecdote with you.
I have 4 wonderful daughters and if you knew me personally you’d know any opportunity I have to talk about any of them, I will. You’ll hear me talking about them at the ballgame, at the supermarket, and Home Depot. In fact, at ONC we have these long hallways and I sometimes see my colleagues diving into their offices as I stroll down them in order to avoid seeing “the slide show” on my phone or hearing the “funny anecdote” about the Washington kids.
But I think this time, here today, I’ll tell you a relevant story about my kids.
I had the ultimate proud papa moment in the summer of 2013 when my twin daughters, Kayla and Kristine, enrolled at my medical school alma mater. The highest degree of anxiety that I have heard from my kids about school was not what I thought. No tears about biochemistry. No tears about anatomy. No tears about physiology. Even no tears about using Epic Systems, the University of Virginia’s EMR.
But when they went to outside rotations, where the providers were documenting on paper, their anxiety level was off the charts! This is all to say that the next generation of physicians, which includes my daughters, has no concept of caring for patients without electronic health records and technology – only an expectation that the technology will improve, will make their practice better, and will meet the promise of health IT in healthcare. And it’s because I am able to view this world through my daughters’ eyes, and now from my seat at ONC, I am able to say to you today that our technology journey hasn’t been perfect, and it won’t be perfect. But the great strides we have made, in a few short years, are truly remarkable. And I can’t imagine us going back.